
What Is GDM and Why Does It Matter?
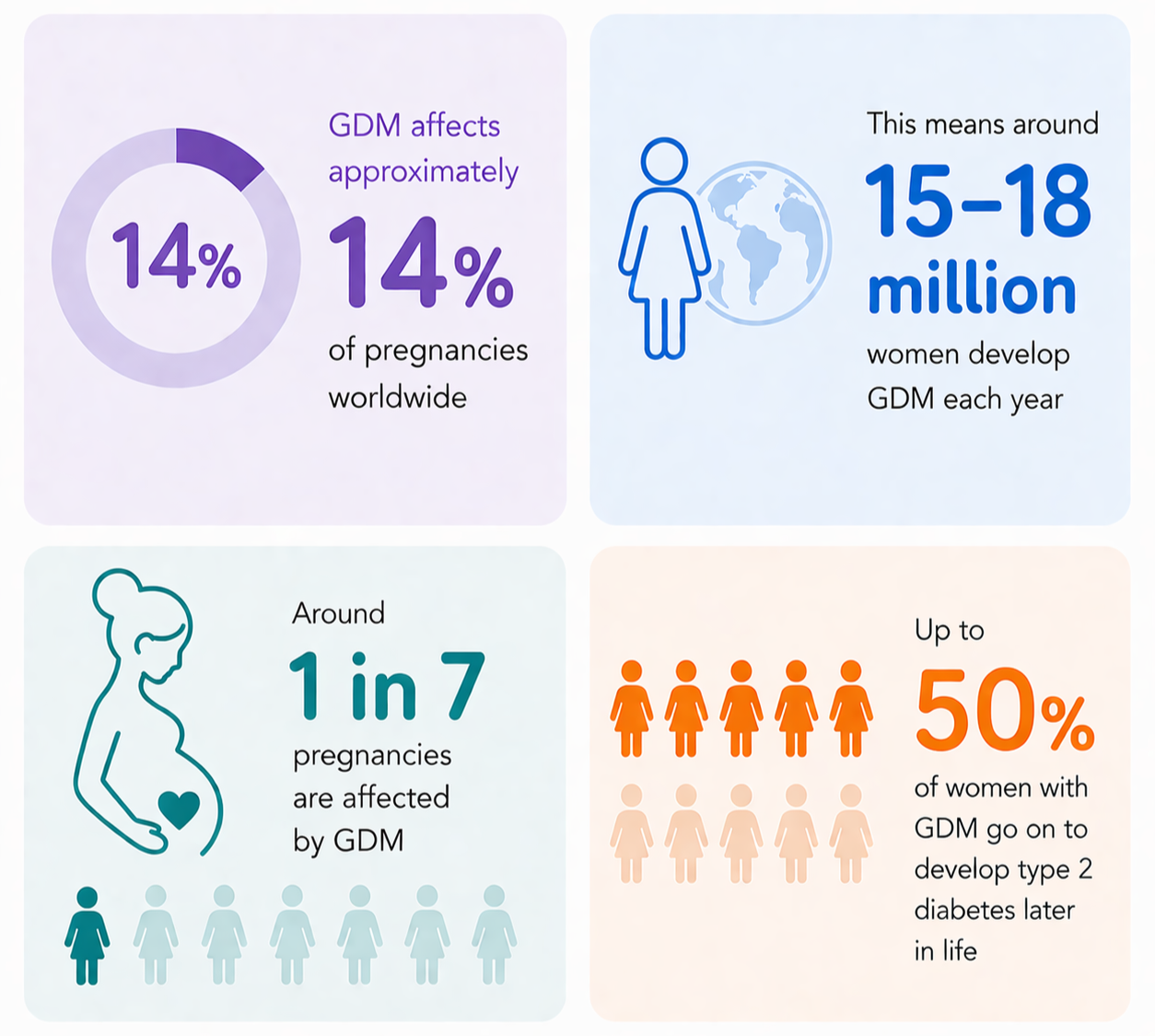
The World Health Organization reports that around 21 million women are affected by diabetes in pregnancy globally, of which the majority of cases are GDM. This means around 15-18 million women are diagnosed with GDM each year.
What is GDM? Gestational diabetes mellitus (GDM) is a condition that develops during pregnancy, where blood glucose levels become higher than normal. This happens when hormones produced by the placenta interfere with the body’s ability to use insulin effectively, resulting in insulin resistance. The exact cause of GDM is not fully understood but hormonal changes during pregnancy play a key role in disrupting normal glucose regulation, and in most cases, glucose levels return to normal after delivery.
GDM at a Glance
So, Why Does it Matter?
Risks During Pregnancy and Beyond
The complications of GDM are often manageable, particularly if blood glucose levels are carefully monitored and controlled from the time of diagnosis. If not well managed, GDM can lead to complications during pregnancy and delivery, including:
Increased risk of stillbirth
Pre-eclampsia (Pregnancy complication due to high blood pressure)
Macrosomia (Larger than average baby)
Neonatal hypoglycaemia (Low blood sugar in newborn baby)
Preterm birth
Despite usually resolving after delivery, GDM can have lasting implications. Women who have been diagnosed with GDM are at higher risk of developing Type 2 diabetes later in life, with up to 50% going on to develop the condition, as well as cardiovascular disease. This highlights that GDM is not just a short-term complication, but an early indicator of future health risk.
Rising Pressure on Health Services
Rates of GDM are increasing worldwide, in part due to the rising prevalence of obesity amongst women of reproductive age. Obesity is a major risk factor for GDM, as it contributes to insulin resistance during pregnancy. As more women are diagnosed with GDM, the demand for healthcare support continues to grow. Many require regular blood glucose monitoring, specialist care, and postpartum follow-up to reduce the risk of developing Type 2 diabetes. This increasing demand is placing additional pressure on maternity services, diabetes care, and wider public health systems both during pregnancy and in the years that follow.
Health Inequalities and Disparities
GDM does not affect all women equally. It is more common amongst women from certain ethnic backgrounds, including South Asian, Black, Hispanic, and Middle Eastern populations. For women living in socioeconomically disadvantaged areas, the inequality is less about risk than about detection: they are more likely to face barriers to screening and follow-up, and GDM can go undiagnosed and unmanaged even when it is present.
These disparities reflect broader gaps in access to care. Some women struggle to access screening and diagnosis during pregnancy whilst others lack clear health information or the ongoing support needed to manage GDM and lower their long-term risk of Type 2 diabetes.
A Window for Early Prevention
GDM represents an important opportunity for early intervention. Pregnancy and the postpartum period provide a key window to identify women at higher risk of developing Type 2 diabetes. With the right support in place, it is possible to reduce this risk and improve long-term health outcomes. Taking action during this time can have lasting benefits for women, their families, and the wider healthcare system.
Why This Matters Now
What sets GDM apart is the opportunity it presents. At a population level, it is one of the clearest early indicators of future Type 2 diabetes. Yet too often, care ends at birth. Continuing to support women after pregnancy, through better screening, clearer information, and consistent follow up, can lower that risk and improve their health in the years that follow.
It is also a chance to reduce inequality. The women least likely to be screened, diagnosed, and supported are often those who stand to benefit most, so improving care after pregnancy can help close those gaps rather than let them widen. Treated as the start of ongoing support rather than the end of care, GDM offers a real opportunity to improve outcomes for women and their families.
References
American Diabetes Association (2024). Standards of Care in Diabetes.
Centers for Disease Control and Prevention (2022). Gestational Diabetes and Type 2 Diabetes.
International Diabetes Federation (2021). IDF Diabetes Atlas.
Johns Hopkins Medicine (n.d.) Gestational diabetes.
National Health Service (2023). Gestational diabetes.
National Institute for Health and Care Excellence (2020). Diabetes in pregnancy: management (NG3).
National Institute of Diabetes and Digestive and Kidney Diseases (2022). Gestational Diabetes.
UK Health Security Agency. Health inequalities and obesity reports.
World Health Organization (2013). Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy.
World Health Organization (2021). Obesity and overweight.
World Health Organization (2025). Hyperglycaemia in pregnancy guidance.
World Health Organization. Diabetes in pregnancy.
World Health Organization. Diabetes prevention and control.
World Health Organization. Social determinants of health.
Wang, H., et al. (2022). Estimation of global and regional gestational diabetes prevalence. Diabetes Research and Clinical Practice.